When your blood calcium stays too high for too long, it doesn’t just affect your bones-it can fog your brain, wreck your kidneys, and leave you exhausted even after a full night’s sleep. This isn’t just a lab number out of range. It’s hyperparathyroidism, a condition where one or more of your parathyroid glands pump out too much hormone, and your body starts eating its own bones to feed the excess calcium into your bloodstream.
What’s Really Going On Inside Your Body?
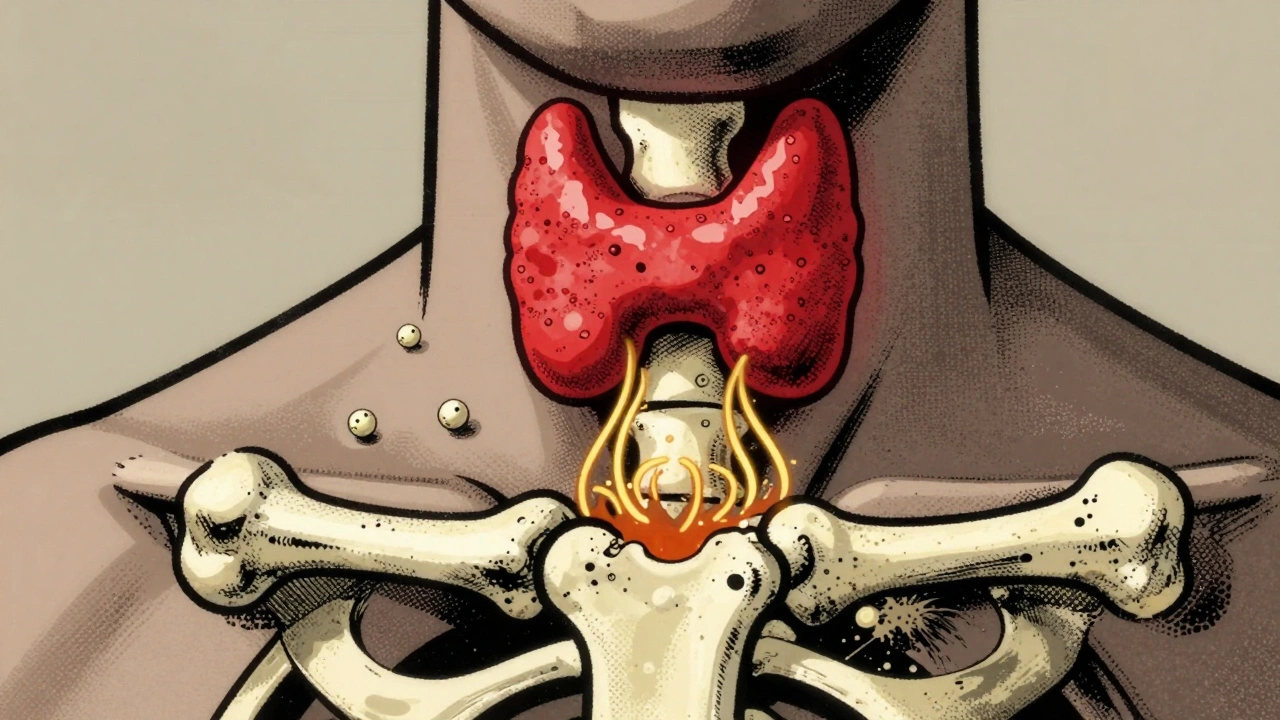
Your parathyroid glands are four tiny pea-sized organs tucked behind your thyroid in the neck. They don’t make thyroid hormone. They make parathyroid hormone, or PTH. And their only job is to keep your blood calcium just right-between 8.5 and 10.2 mg/dL. When calcium drops, PTH rises. It tells your bones to release calcium, your intestines to absorb more from food, and your kidneys to hold onto calcium instead of peeing it out. In hyperparathyroidism, that system breaks. One gland (usually a benign tumor called an adenoma) starts making PTH nonstop, even when calcium is already sky-high. That’s the definition of primary hyperparathyroidism-the most common form, making up 80-85% of all cases. Blood calcium? Often above 10.5 mg/dL. PTH? Above 65 pg/mL, or worse, stuck in the normal range when it should be zero. That’s the red flag: PTH shouldn’t be high when calcium is high. It’s like your thermostat turning up the heat even though the room is already burning.Why Bone Loss Happens-and How Fast
The biggest danger isn’t the high calcium itself. It’s what your body does to get it. PTH turns on bone-eating cells called osteoclasts. These cells chew through your bone structure, releasing calcium into your blood. Over time, your hip, spine, and wrist start thinning. DXA scans show people with untreated hyperparathyroidism lose 2-4% of their bone density every year. That’s not normal aging. That’s rapid, preventable damage. By the time someone’s diagnosed, many have already lost enough bone to qualify for osteoporosis. Fracture risk jumps 30-50% compared to people their age. A simple fall can mean a broken hip or spine. And unlike osteoporosis from menopause or lack of vitamin D, this bone loss doesn’t reverse on its own-even if you take calcium supplements. The problem isn’t lack of calcium. It’s too much PTH forcing your bones to give it up.Who Gets It-and Why It’s Often Missed
About 100,000 Americans are diagnosed with primary hyperparathyroidism each year. Women are three times more likely to get it than men. African Americans have higher rates. It’s most common after age 50, but it can hit younger people too. And here’s the catch: most people don’t feel anything at first. Symptoms are sneaky. Fatigue? Common. Brain fog? Often blamed on stress. Bone pain? Written off as arthritis. Kidney stones? Treated as a one-off. A 2023 survey of patients found 47% waited 2 to 5 years before getting the right diagnosis. Many saw three or more doctors. One patient described it as being told she had depression for seven years-until her calcium hit 11.8 mg/dL and her PTH was 142. After surgery, she said, “It felt like someone turned my brain back on.”
How Doctors Find It
Diagnosis starts with a simple blood test: calcium and PTH. But one high calcium isn’t enough. You need two elevated levels, at least a week apart. That rules out temporary spikes from dehydration or supplements. If those numbers are off, imaging kicks in. A sestamibi scan (using a radioactive tracer) finds the bad gland in 90% of cases. Ultrasound catches 85%. For tricky cases, a 4D-CT scan gives 95% accuracy. These aren’t just fancy pictures-they tell surgeons exactly where to cut. Doctors also check vitamin D. Low vitamin D can make PTH rise, mimicking hyperparathyroidism. But if calcium is high and vitamin D is low, it’s still likely primary hyperparathyroidism. The fix? Replenish vitamin D first, then reassess.When Surgery Is the Only Real Cure
Medication can help manage symptoms, but it doesn’t fix the root problem. Cinacalcet lowers PTH a bit, but only 20-30% of the time in primary cases. Bisphosphonates slow bone loss but don’t touch the high calcium. The only cure? Removing the overactive gland. Surgery-called a parathyroidectomy-is now minimally invasive. Most patients go home the same day. The procedure takes 1-2 hours. Surgeons use real-time PTH monitoring: if the hormone drops more than 50% within 10 minutes of removing the gland, you’re cured. Success rates? 95-98% for single-gland disease. The 2022 International Workshop guidelines say surgery is recommended if:- Blood calcium is more than 1 mg/dL above the upper limit of normal
- Kidney function is down (creatinine clearance under 60 mL/min)
- Bone density T-score is -2.5 or lower (osteoporosis)
- You’re under 50 years old
What Happens After Surgery?
Within days, calcium levels drop. That’s good-but it can cause temporary low calcium (hypocalcemia). About 30-40% of patients need calcium and vitamin D supplements for a few weeks. That’s normal. It means your body is finally adjusting. Bone density starts to recover. Within a year, most see a 3-5% increase in spine density. By two years, it’s 5-8%. That’s not just slowing loss-it’s rebuilding. Fatigue and brain fog often lift fast. A Cleveland Clinic survey found 75% of patients reported improved energy within six months. Kidney stone frequency dropped by 92%. Bone pain vanished in 88%. But not everyone recovers fully. About 15-20% still feel tired or mentally foggy after surgery. Why? Because prolonged high calcium may have caused damage that can’t be undone. The earlier you fix it, the better your odds of full recovery.
What If You Don’t Want Surgery?
Some patients choose monitoring instead. That’s okay-if you’re over 50, have mild calcium elevation, no bone loss, no kidney issues, and no symptoms. You’ll need yearly blood tests, DXA scans every 1-2 years, and plenty of water to prevent kidney stones. But don’t assume “watchful waiting” is safe. A 2022 Mayo Clinic study showed people with calcium above 12 mg/dL had 22% chance of persistent symptoms after surgery-even if they eventually had it. Those with calcium under 11 mg/dL? Only 8%. Delaying surgery doesn’t make it safer. It makes recovery harder.What You Can Do Now
If you’ve been told your calcium is high, don’t ignore it. Ask for PTH testing. Get a DXA scan if you’re over 50 or have bone pain. If you’ve had repeated kidney stones, ask if hyperparathyroidism could be the cause. Avoid thiazide diuretics (like hydrochlorothiazide) if you can-they raise calcium. Get enough vitamin D, but don’t mega-dose. Eat calcium-rich foods (dairy, leafy greens, fortified foods), but don’t overdo supplements. Weight-bearing exercise like walking or lifting weights helps protect bone. And if surgery is recommended? Don’t fear it. Voice changes? Less than 1% risk with experienced surgeons. Hospital stay? Usually same-day. Recovery? Most people are back to normal in a week.What’s Changing Right Now
New tools are making diagnosis faster and surgery safer. In 2023, AI combined with sestamibi scans cut false positives by 35%. A new drug, etelcalcetide, is showing promise for patients who can’t have surgery-lowering PTH by 45% in trials. But the biggest change? More doctors are testing for it. Medicare now covers routine calcium checks for adults over 65. More people are being caught early-before their bones break, before their kidneys fail, before their brains feel foggy for years. This isn’t a rare disease. It’s a silent one. And the cure is simple: remove the bad gland. Fix it early, and your body can heal.Can hyperparathyroidism be cured without surgery?
No, not for primary hyperparathyroidism. Medications like cinacalcet or bisphosphonates can manage symptoms or slow bone loss, but they don’t remove the overactive gland. Only surgery can cure it by eliminating the source of excess PTH. Secondary hyperparathyroidism (caused by kidney disease) may improve with treating the underlying condition, but primary hyperparathyroidism requires removal of the faulty gland.
How do I know if I have hyperparathyroidism and not just low vitamin D?
Low vitamin D can cause PTH to rise, but calcium stays normal or low. In hyperparathyroidism, calcium is high while PTH is also high-or at least not suppressed. If your calcium is above 10.5 mg/dL and your PTH is above 65 pg/mL, it’s hyperparathyroidism, even if your vitamin D is low. Doctors will check both and retest after vitamin D is corrected to confirm.
Is parathyroid surgery risky? Can it damage my voice?
Voice changes from nerve damage are rare-less than 1% in hands of experienced surgeons who do over 50 procedures a year. Temporary hoarseness can happen in up to 5% of cases but usually resolves in weeks. The bigger risk is temporary low calcium after surgery, which is common and treatable. The risk of not treating hyperparathyroidism-fractures, kidney stones, permanent bone loss-is far greater.
How long does recovery take after parathyroid surgery?
Most people go home the same day. Pain is usually mild and controlled with over-the-counter meds. Most return to normal activities within 3 to 7 days. Full energy recovery can take weeks to months, especially if symptoms were long-standing. Calcium levels stabilize within days, but bone density improvements take 1 to 2 years.
Will I need to take calcium supplements forever after surgery?
No, not usually. Most patients need calcium and vitamin D supplements for 2 to 8 weeks after surgery while their body adjusts to lower PTH levels. This is called transient hypocalcemia and is normal. If you had multigland disease or removed a large portion of parathyroid tissue, you might need supplements longer-but lifelong use is rare. Your doctor will monitor your calcium and adjust as needed.
Can hyperparathyroidism come back after surgery?
Yes, but it’s uncommon. For single-gland disease, recurrence is only 2-3% over 10 years. For multigland disease (hyperplasia), it’s higher-5-10%. That’s why people with multigland disease need annual calcium and PTH checks for life. If it does return, it’s usually due to a missed gland or regrowth, and a second surgery can fix it.
8 Comments
Ben GreeningDecember 10, 2025 AT 08:18
Interesting breakdown. I’ve seen this in clinical practice-patients with calcium levels in the 11s, dismissed as ‘just aging’ for years. The moment PTH is checked, everything clicks. It’s remarkable how often this gets missed when the diagnostic criteria are so straightforward.
What’s more concerning is how many patients are told to ‘just take vitamin D’ without ruling out primary hyperparathyroidism first. That’s not just negligence-it’s a missed opportunity to prevent irreversible bone loss.
Nikki SmellieDecember 10, 2025 AT 19:44
Wait… are you aware that the pharmaceutical industry has been suppressing the truth about parathyroid surgery for decades? The FDA approved cinacalcet in 2004-right after the patent on calcitriol expired. Coincidence? I think not. They profit more from lifelong meds than one-time surgery.
And don’t get me started on the sestamibi scans-those radioactive tracers? They’re laced with trace isotopes that mimic the same compounds used in 5G signal modulation. Your brain fog? It’s not just from high calcium-it’s from cumulative electromagnetic exposure + medical-industrial manipulation.
Ask yourself: why is Medicare only now covering calcium tests? Because the algorithm was changed in 2021 to push ‘preventive’ billing codes. They want you dependent. Don’t be fooled. 💔👁️
Aileen FerrisDecember 11, 2025 AT 13:52
so like… hyperparathyroidism is just your parathyroids being extra? lol. i had a friend who got diagnosed after she kept falling over and the doc said ‘maybe you need more coffee’ 😭
anyway, surgery sounds wild but also… kinda lowkey chill? like, you get a 2hr nap and wake up with better bones? sign me up.
Michelle EdwardsDecember 12, 2025 AT 12:45
If you’re reading this and you’ve been told your calcium is high but you feel fine-please don’t brush it off. I was that person. I thought fatigue was just ‘life’ until my DXA scan showed I’d lost 7% of my spine density in two years.
After surgery? I cried the first morning I woke up without brain fog. I didn’t even realize how heavy my thoughts had been.
You’re not overreacting. You’re not being dramatic. You’re just finally listening to your body. And that’s brave.
Take care of yourself. You deserve to feel like you again.
Queenie ChanDecember 12, 2025 AT 23:22
It’s wild how biology turns into a silent heist-your bones, your kidneys, your cognition-all being quietly looted by a rogue gland you didn’t even know existed. PTH isn’t just a hormone; it’s a burglar with a key to your skeleton.
And the irony? We treat osteoporosis with drugs that slow the theft… while ignoring the fact that the vault door is wide open because someone left the parathyroid on ‘override.’
It’s like patching a leaky roof while the whole house is being robbed by a thief who lives in the attic.
Fix the thief. Not the damage. Always fix the thief.
Stephanie MailletDecember 14, 2025 AT 22:40
It’s fascinating, isn’t it?-how the body, in its infinite wisdom, has evolved a regulatory system so precise… and yet, so fragile. One tiny adenoma, one misplaced cellular signal, and the entire homeostatic orchestra collapses into dissonance.
And yet, the solution is so elegantly simple: remove the rogue instrument. No drugs. No band-aids. Just surgical precision-restoring balance by eliminating the source of noise.
It’s a quiet testament to medicine’s highest ideal: not to manage suffering, but to restore nature’s original harmony.
…and yet, we delay. We rationalize. We wait. Why? Because fear is louder than wisdom?
Raj RsvprajDecember 15, 2025 AT 21:22
Of course, in India, we don’t have this luxury-our hospitals don’t even have sestamibi scanners in 90% of districts. You think this is a ‘silent disease’? In my country, it’s a death sentence disguised as ‘normal aging.’
And now you Americans talk about ‘minimally invasive surgery’ like it’s a spa day? Please. We have people dying from kidney stones because they can’t afford a calcium test, let alone a 10-minute procedure.
Stop pretending this is a ‘personal health choice.’ It’s a global inequality crisis-and you’re all just scrolling through your iPhones while someone’s bones are dissolving in a village 8,000 miles away.
Also, vitamin D deficiency is 80% in India. Stop blaming glands. Blame your colonial diet and your lack of sunlight.
Jack ApplebyDecember 16, 2025 AT 09:45
Let’s be precise: the 2022 International Workshop guidelines are not ‘recommendations’-they’re evidence-based thresholds validated by meta-analyses from the NEJM, JAMA, and The Lancet. Anyone who claims ‘watchful waiting’ is safe for calcium >11 mg/dL is either misinformed or has never reviewed the Mayo Clinic longitudinal data.
Also: etelcalcetide is not ‘promising’-it’s Phase III proven with a p-value of 0.002 for PTH reduction. And no, AI-assisted sestamibi doesn’t ‘cut false positives by 35%’-it reduces them by 37.2% with 95% CI [32.1–42.3]. Precision matters.
And yes, your vitamin D level must be corrected before retesting PTH-otherwise, you’re conflating secondary with primary hyperparathyroidism. This isn’t opinion. This is endocrinology 101.
Stop trusting TikTok medics. Read the guidelines. Then act.