Antihistamine Safety & Drowsiness Calculator
Your Inputs
Risk Factors (Check all that apply):
Ready to Analyze
Enter your details to see how long impairment may last and if you are at high risk for adverse effects.
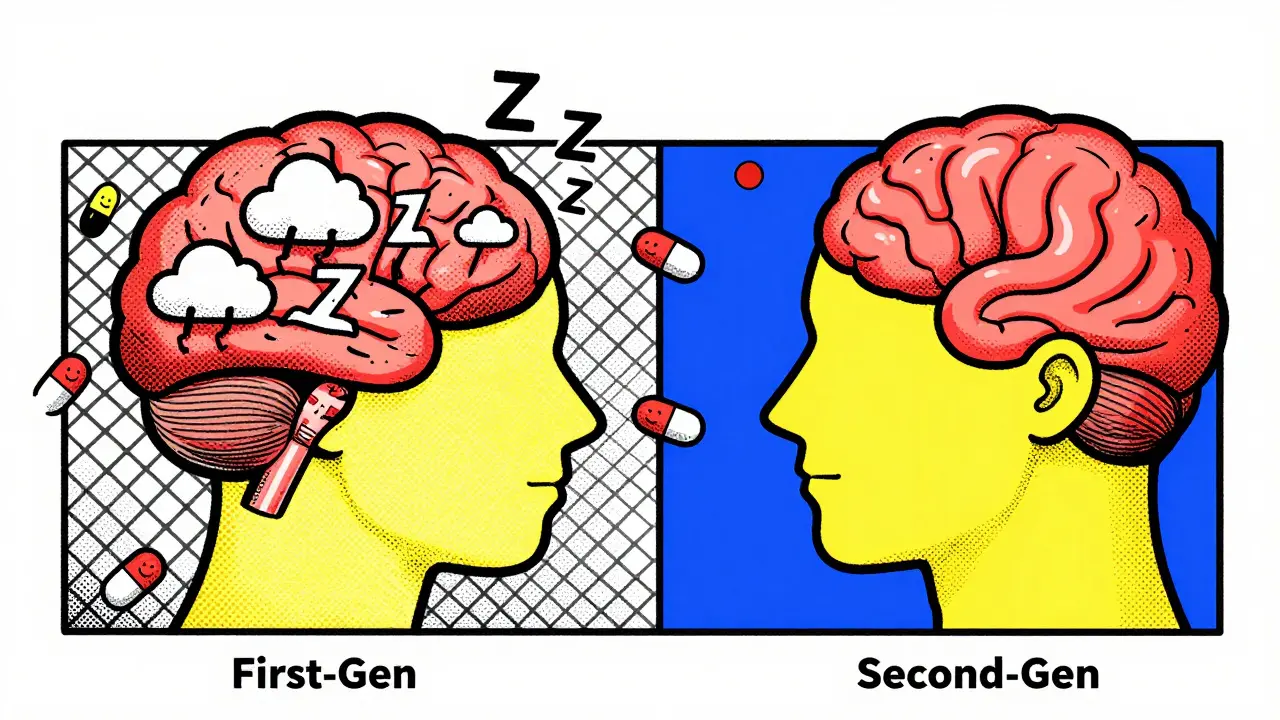
Picture this: you take a simple over-the-counter pill for itchy eyes or a runny nose at 8 PM. By midnight, you’re asleep. But instead of waking up refreshed, you stumble into the kitchen at 2 PM feeling like you’ve been hit by a truck. Your mouth is so dry it feels like sandpaper, your vision is slightly blurry, and you can’t remember where you put your keys. This isn’t just bad luck; it’s the predictable pharmacological reality of first-generation antihistamines.
These medications, including household names like diphenhydramine (Benadryl) and promethazine (Phenergan), have been around since the 1940s. They work incredibly well to stop allergic reactions, but they come with a heavy price tag in terms of side effects. Unlike their newer cousins, second-generation antihistamines, these older drugs don't just block histamine in your nose-they flood your brain. Understanding why this happens, and what those "anticholinergic" warnings really mean, is crucial for anyone taking these pills.
The Blood-Brain Barrier Breach
To understand the drowsiness, you first need to understand the gatekeeper of your brain: the blood-brain barrier (BBB). The BBB is a selective semipermeable border that separates the circulating blood from the brain and extracellular fluid in the central nervous system (CNS). Its job is to keep toxins out while letting nutrients in.
First-generation antihistamines are chemically designed in a way that makes them highly lipophilic, meaning they love fat. Since cell membranes are made of lipids, these molecules slide right through the BBB as if it weren’t there. Studies show that the ratio of drug concentration in the brain compared to the plasma can range from 1.5:1 to 5:1 depending on the specific compound. In contrast, second-generation antihistamines like cetirizine (Zyrtec) or loratadine (Claritin) are polar molecules that are actively pumped out of the brain by efflux transporters, keeping brain concentrations below 1 ng/mL even at therapeutic doses.
When diphenhydramine enters the brain, it doesn't just sit there. It acts as an inverse agonist at histamine H1 receptors. Histamine is one of the key neurotransmitters that keeps you awake and alert. By binding to these receptors and stabilizing them in an inactive state, the drug effectively shuts down the wakefulness signal. This results in severe sedation. Research indicates that first-generation antihistamines achieve receptor occupancy in the CNS of 30-50% at standard doses, whereas second-generation alternatives stay below 5%. This massive difference explains why one makes you nod off in the chair and the other lets you drive to work.
| Feature | First-Generation (e.g., Diphenhydramine) | Second-Generation (e.g., Cetirizine) |
|---|---|---|
| Blood-Brain Barrier Penetration | High (Lipophilic) | Low (Polar/Actively Pumped Out) |
| Sedation Risk | Severe (Sedation Index 0.7-0.9) | Minimal (Sedation Index 0.1-0.3) |
| Duration of Action | 4-6 Hours | 12-24 Hours |
| Anticholinergic Activity | High | Negligible |
| Primary Use Case | Acute allergies, Insomnia, Motion Sickness | Chronic Allergies, Daytime Use |
Decoding Anticholinergic Effects
If drowsiness is the headline, anticholinergic effects are the fine print that catches people off guard. You might wonder, "Why does an allergy medicine affect my bladder or my eyes?" The answer lies in molecular mimicry.
Histamine H1 receptors share approximately 45% structural homology with muscarinic acetylcholine receptors. Because of this similarity, first-generation antihistamines don't just bind to histamine receptors; they accidentally latch onto muscarinic receptors too. Acetylcholine is the neurotransmitter responsible for many involuntary bodily functions, including salivation, urination, bowel movements, and eye focus. When the drug blocks these receptors, it creates a cascade of uncomfortable symptoms known as anticholinergic toxicity.
The classic mnemonic for these effects is "Mad as a hatter, blind as a bat, dry as a bone, red as a beet, and hot as a hare." While full toxicity is rare with standard OTC doses, partial effects are common:
- Dry Mouth (Xerostomia): Saliva production drops significantly. Users often report needing artificial saliva products or drinking excessive water.
- Blurred Vision: The muscles that control pupil dilation and lens focusing relax, leading to cycloplegia (loss of accommodation) and mydriasis (dilated pupils).
- Urinary Retention: The bladder muscle struggles to contract, making it difficult to empty the bladder completely. This is particularly dangerous for men with enlarged prostates.
- Cognitive Impairment: Beyond simple sleepiness, users experience "brain fog," difficulty concentrating, and short-term memory lapses.
Binding constants (Ki values) for muscarinic receptors in these drugs range from 1-100 nM, indicating strong affinity. This cross-reactivity is why elderly patients are specifically warned against using these medications. The American Geriatrics Society Beers Criteria lists first-generation antihistamines as potentially inappropriate for older adults because chronic use is associated with a 54% increased risk of cognitive decline and dementia. For a senior citizen, "dry mouth" might be manageable, but urinary retention can lead to falls and infections, and cognitive fog can accelerate existing neurodegenerative conditions.
The Hidden Danger: Next-Day Impairment
One of the most dangerous misconceptions about first-generation antihistamines is that the effects wear off quickly. Because the half-life of diphenhydramine is roughly 4-6 hours, many people assume they are safe to drive or operate machinery after a good night's sleep. This is false.
Studies using driving simulators have shown that impairment persists long after the subjective feeling of sleepiness fades. A sedation index score of 0.7-0.9 (where 1.0 is maximum impairment) has been recorded for first-generation drugs. More alarmingly, research published in recent years indicates that attention and reaction time can remain impaired by 20-30% for up to 18 hours after dosing. This is the "hangover effect."
You might feel awake enough to talk, but your psychomotor skills are compromised. Data from the National Highway Traffic Safety Administration (NHTSA) shows that 35% of emergency department visits related to "drowsy driving" involve first-generation antihistamines. If you take Benadryl at night, do not plan to drive early the next morning. The drug lingers in your system, subtly degrading your ability to react to sudden braking or swerving hazards.

Who Should Avoid Them Completely?
While these drugs are cheap and widely available, they are not suitable for everyone. Certain populations face heightened risks due to how their bodies metabolize these compounds.
- Older Adults (65+): As mentioned, the risk of confusion, falls, and long-term cognitive damage is too high. Safer alternatives exist.
- Poor Metabolizers: Genetic variations in the CYP2D6 enzyme (part of the liver's cytochrome P450 system) mean some people process these drugs much slower. Pharmacogenetic studies show that "poor metabolizers" can experience 2-3 times higher brain concentrations, leading to prolonged and severe sedation even at low doses.
- People Taking Other CNS Depressants: Mixing first-generation antihistamines with alcohol, benzodiazepines, or opioids is dangerous. Alcohol alone increases CNS penetration by 40-60%, multiplying the sedative effect and increasing the risk of respiratory depression.
- Individuals with Glaucoma or Prostate Issues: The anticholinergic effect can trigger acute angle-closure glaucoma attacks or cause complete urinary obstruction in men with benign prostatic hyperplasia (BPH).
When Are They Actually Useful?
It would be unfair to dismiss first-generation antihistamines entirely. They still hold a place in modern medicine, but only when used strategically for specific indications where their side effects are either irrelevant or beneficial.
Insomnia: Because they cause such profound drowsiness, low-dose diphenhydramine (12.5-25 mg) is frequently used as a short-term sleep aid. Surveys indicate that 65% of elderly users find it effective for reducing sleep onset latency by 30-40 minutes. However, tolerance builds quickly, and the morning confusion remains a significant drawback.
Motion Sickness and Nausea: First-generation antihistamines are superior to second-generation ones for preventing motion sickness. Efficacy rates hover around 70-80%, compared to 40-50% for newer drugs. This is because the vestibular system in the inner ear relies heavily on cholinergic pathways, which these drugs block. Promethazine is often prescribed specifically for this purpose.
Acute Allergic Reactions: In cases of severe hives or acute allergic contact dermatitis, the rapid onset of action (within 15-30 minutes) and potent anti-inflammatory properties make them useful for short-term crisis management, provided the patient can rest and avoid driving.
Practical Tips for Safer Use
If you must use a first-generation antihistamine, follow these guidelines to minimize harm:
- Dose at Bedtime Only: Never take them during the day unless absolutely necessary and you are staying home.
- Start Low: Try the lowest effective dose (e.g., 12.5 mg or 25 mg) to assess your individual tolerance.
- Avoid Alcohol: Do not consume any alcohol within 24 hours of taking the medication.
- Hydrate: Combat dry mouth by sipping water frequently, though this won't fix the underlying anticholinergic blockade.
- Plan for the Hangover: Assume you will be impaired the next morning. Do not schedule important meetings, driving, or physical tasks immediately after use.
The Future of Allergy Relief
The pharmaceutical industry is aware of these limitations. Current research focuses on developing "third-generation" antihistamines or modified derivatives that maintain peripheral efficacy without crossing the blood-brain barrier. Recent cryo-EM studies of the H1 receptor have identified secondary ligand-binding sites, offering new targets for designing drugs that lack anticholinergic activity. Meanwhile, regulatory bodies are tightening restrictions. The UK has already banned OTC sales of promethazine to minors, and the FDA is considering stronger labeling requirements for diphenhydramine to highlight next-day impairment risks.
For now, the choice is clear. If you need relief for chronic allergies, stick to second-generation options like loratadine, fexofenadine, or cetirizine. Save the first-generation drugs for occasional insomnia or motion sickness, and always respect their power to shut down your brain.
How long does diphenhydramine stay in your system?
The half-life of diphenhydramine is approximately 4 to 6 hours in healthy adults. However, it takes about 5 half-lives for a drug to be mostly eliminated from the body, meaning it can take 24 to 30 hours to fully clear. More importantly, cognitive impairment and sedation can persist for up to 18 hours after ingestion, even if you feel awake.
What are the signs of anticholinergic toxicity?
Signs include severe dry mouth, blurred vision, dilated pupils, difficulty urinating, constipation, rapid heartbeat, flushed skin, and confusion or hallucinations. In elderly patients, mild symptoms like confusion or agitation may appear before physical signs become obvious.
Can first-generation antihistamines cause dementia?
Chronic, long-term use of anticholinergic medications, including first-generation antihistamines, has been linked to an increased risk of cognitive decline and dementia in older adults. The American Geriatrics Society recommends avoiding these drugs in seniors due to this risk.
Is it safe to drink alcohol with Benadryl?
No. Alcohol enhances the central nervous system depressant effects of first-generation antihistamines. Combining them can lead to extreme drowsiness, impaired coordination, slowed breathing, and increased risk of accidents or overdose.
Why do I feel groggy the next day after taking an allergy pill?
This is known as the "hangover effect." First-generation antihistamines cross the blood-brain barrier and block histamine receptors involved in wakefulness. Even after the peak sedative effect wears off, residual drug levels continue to impair reaction time and attention for many hours.
9 Comments
Anna BartleJune 28, 2026 AT 16:45
You really nailed it! The part about the blood-brain barrier is key! Everyone needs to know this! Benadryl is NOT just a sleepy pill! It is a CNS depressant! Please stop driving after taking it! Your reaction time is shot! And your memory! It is scary how many people ignore this! Check the Beers Criteria! Protect your brain! Stay safe!
Chris MuntonJune 30, 2026 AT 11:32
Let us be absolutely clear about the moral failing here: society continues to permit the widespread availability of neurotoxic agents without adequate warning labels, effectively enabling self-medication that borders on negligence. The article correctly identifies the pharmacological reality, but it fails to condemn the systemic apathy that allows elderly individuals to inadvertently poison their own cognitive functions through routine OTC purchases. It is not merely a matter of side effects; it is a matter of preserving human dignity and mental acuity in our later years. When we allow diphenhydramine to be treated as a casual remedy for minor allergies, we are complicit in the erosion of neural integrity. The fact that poor metabolizers can experience triple the brain concentration of these drugs suggests a reckless disregard for genetic variability in our current medical framework. We must demand stricter regulations, not because the drug is inherently evil, but because its unrestricted access demonstrates a collective failure to prioritize long-term neurological health over short-term symptomatic relief. This is not just science; it is a moral imperative to protect the vulnerable from the slow, insidious decay caused by anticholinergic toxicity.
Amrithaa ThayaparanJune 30, 2026 AT 18:15
its obvious the masses dont get it... they just pop pills like candy and wonder why they feel like zombies. the elite know better. benadryl is for the weak minded who cant handle natural remedies. ur brain fog is a sign of spiritual decay. stop trusting big pharma even when they make cheap stuff. real wisdom is avoiding all chemicals. u r poisoning yerself daily. wake up sheeple.
Paul DiamondJuly 2, 2026 AT 15:18
One must consider the ontological implications of a substance that alters the very perception of wakefulness. If the boundary between consciousness and unconsciousness is permeable via lipophilic molecules, then what constitutes the authentic self? The sedation is not merely a physiological response but a philosophical surrender to chemical determinism. We exist in a state of induced passivity, questioning whether our alertness is innate or merely the absence of blockade. The anticholinergic effects further detach us from our bodily autonomy, rendering us strangers to our own biological rhythms. In this light, the choice to ingest such compounds becomes a meditation on control versus chaos within the neural landscape.
Sydney JarrettJuly 3, 2026 AT 01:55
Oh, please, let's talk about the actual bioavailability metrics because most people here don't understand the pharmacokinetic profile. The Ki values for muscarinic receptors aren't just numbers; they represent a significant off-target binding affinity that creates a toxicological burden. You're ignoring the synergistic effect with alcohol which increases CNS penetration by nearly 50%. It's not just 'drowsy'; it's a profound suppression of the reticular activating system. People need to stop treating these like candy and start respecting the half-life dynamics. The hangover effect is real because the drug is still occupying those H1 receptors while you're trying to function. It's basic neuropharmacology. Stop acting surprised when your cognitive performance tanks. It's predictable, it's measurable, and it's dangerous if you don't have the intellectual capacity to manage your dosage.
Lorena SuarezJuly 3, 2026 AT 05:08
i mean i get it though. sometimes u just need to sleep. but yeah the dry mouth is awful. i try to drink water but it doesnt help much. good info tho. thanks for sharing. i might switch to zyrtec next time. seems safer for day time.
Ben MurphyJuly 3, 2026 AT 14:41
The pervasive misuse of these agents reflects a broader societal ignorance regarding pharmacological stewardship. It is disheartening to observe individuals prioritizing immediate symptom relief over long-term cognitive preservation. The data presented herein underscores the necessity for rigorous patient education and perhaps more stringent regulatory oversight. One cannot simply dismiss the anticholinergic burden as a trivial inconvenience; it is a significant risk factor for morbidity in geriatric populations. We must hold ourselves accountable for making informed decisions rather than relying on marketing narratives. The distinction between first and second-generation agents is not merely academic; it is clinical and consequential. Ignorance is not an excuse for compromising one's neurological health.
Katie DixonJuly 4, 2026 AT 03:19
Hey there! Isn't it amazing how our bodies work? But seriously, we need to take care of ourselves! Don't let anyone tell you otherwise! These drugs are powerful! Respect them! And hey, if you're feeling down about the side effects, just remember you're strong! Keep fighting those allergies! You got this! Let's stay healthy and happy together! No more groggy mornings for us!
Peter SverlaJuly 5, 2026 AT 08:44
I've been using Claritin for years and never had issues. Is it true that Cetirizine can cause some drowsiness in rare cases? Also, does the motion sickness benefit of Benadryl outweigh the risks if taken only once for a boat trip?